Frequently asked questions
Does embryo grading matter?
Yes. Embryo grading gives important clues about implantation potential. However, even lower-graded embryos can result in healthy babies, so grading should never be seen as a guarantee.
Does embryo grading matter if euploid?
It still matters. A euploid embryo (chromosomally normal) may look different under the microscope. Morphology helps predict which euploid embryo has the best chance of attaching to the womb.
Does embryo grading matter with PGT-A?
Yes. PGT-A provides genetic information, while grading provides visual and developmental information. Together, they help doctors decide which embryo to transfer first.
How are embryos graded?
Embryologists examine the blastocyst under a high-powered microscope. They look at three things: the inner cell mass (which becomes the baby), the trophectoderm (which becomes the placenta), and the level of expansion. Each feature is graded from A to D.
How does embryo grading work?
It’s a detailed observation process. Embryologists use international guidelines such as ASEBIR to describe embryo quality clearly and consistently.
What are the embryo grades?
Grades run from A (best) to D (lower quality). Many clinics also use numbers like 4AA or 5AA to show expansion and quality.
What does the number mean in embryo grading?
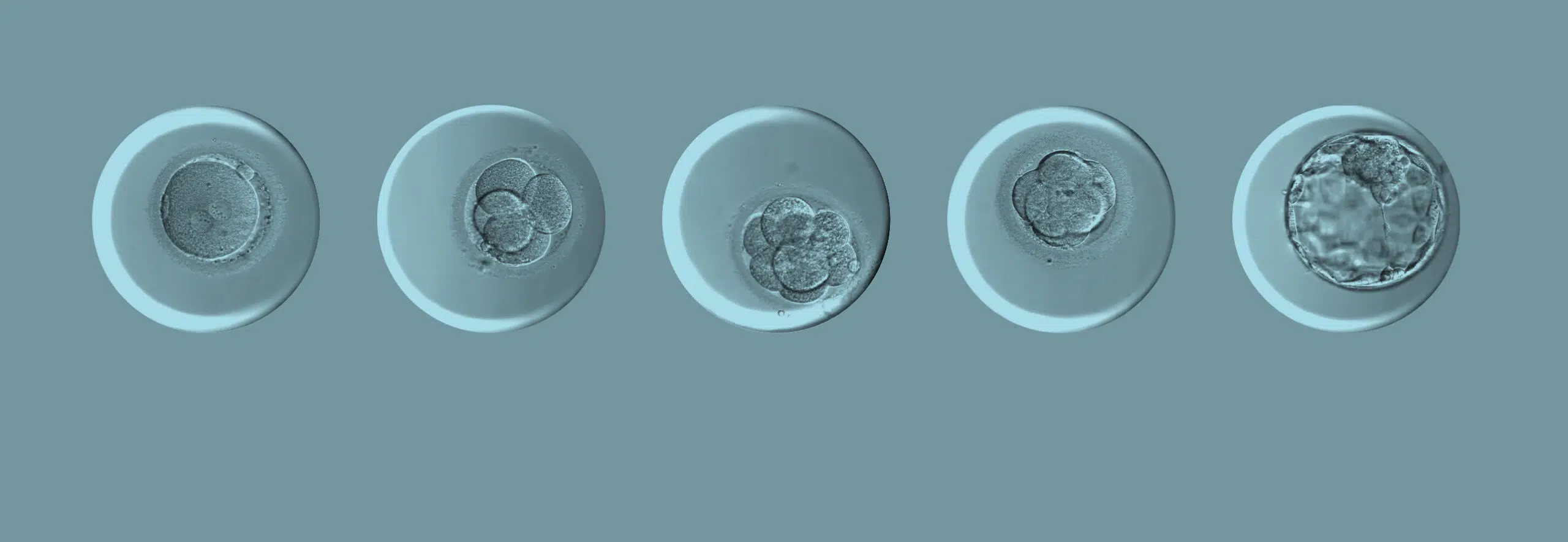
The number shows how expanded the blastocyst is:
1 = early blastocyst
2 = blastocyst
3 = full blastocyst
4 = expanded blastocyst
5 = hatching blastocyst
6 = hatched blastocyst
The letters describe the quality of the inner cell mass and trophectoderm.
When are embryos graded?
Embryos are usually graded on day 5 or 6 after fertilisation, when they reach the blastocyst stage. Some clinics also record early-stage observations on days 2 and 3.
What is a 4AA embryo?
A 4AA embryo is a fully expanded blastocyst with excellent inner cell mass and trophectoderm. It’s considered one of the strongest grades.
What is a 5AA embryo?
A 5AA embryo is beginning to hatch from its shell and has excellent cell quality. It’s often chosen first for transfer or freezing.
Can a lower-graded embryo become a baby?
Yes. Many pregnancies come from embryos graded C, or D. Grading indicates likelihood, not destiny.
Can embryo grading predict miscarriage?
No. Miscarriage risk depends mainly on genetic health and maternal factors. PGT-A provides more insight into chromosomal issues.
What happens if none of my embryos reach blastocyst?
It can feel disappointing, but it doesn’t mean you can’t get pregnant. Your doctor will review stimulation, egg quality, and lab conditions to adjust your next cycle.
Do frozen embryos have lower success rates?
Not anymore. With modern vitrification, frozen embryos have almost the same success rates as fresh ones once thawed.
Does age affect embryo grading?
Yes. Egg quality declines with age, making it more common for embryos to show uneven cell structure or slower growth after 35.
Is AI replacing embryologists?
No. AI supports embryologists by analysing patterns too small for the human eye, but final decisions are always made by experts.